Peptide Weight Loss Protocol: What You Need to Know

A peptide weight loss protocol is the prescribed, clinician-supervised use of GLP-1 receptor agonists, such as semaglutide (Wegovy) or tirzepatide (Zepbound), combined with a reduced-calorie diet and increased physical activity to produce sustained fat loss. These are not supplements you order online. They are prescription incretin-based medicines requiring medical evaluation, stepwise dose escalation, and ongoing monitoring. The protocol structure, not just the peptide itself, is what separates clinical outcomes from guesswork. If you are between 25 and 50 and seriously exploring peptide therapy for weight loss, understanding how these protocols actually work is the difference between results and risk.
What is a peptide weight loss protocol and how does it work biologically?
Peptide weight loss protocols work by targeting hormone receptors that regulate hunger, insulin release, and how fast your stomach empties. GLP-1 (glucagon-like peptide-1) is a naturally occurring gut hormone released after eating. GLP-1 receptor agonists like semaglutide mimic this signal at a sustained level, producing appetite suppression and delayed gastric emptying that reduces caloric intake without requiring willpower alone. This is not direct fat burning. It is hormonal recalibration of your body’s hunger and satiety signals.
The mechanism translates into real metabolic changes. Increased insulin secretion in response to meals improves glucose control. Reduced appetite lowers total caloric intake. Slower gastric emptying extends the feeling of fullness after smaller portions. Together, these effects create a caloric deficit that the body sustains over months, which is why clinical trials measure outcomes at 68 to 72 weeks rather than 12.
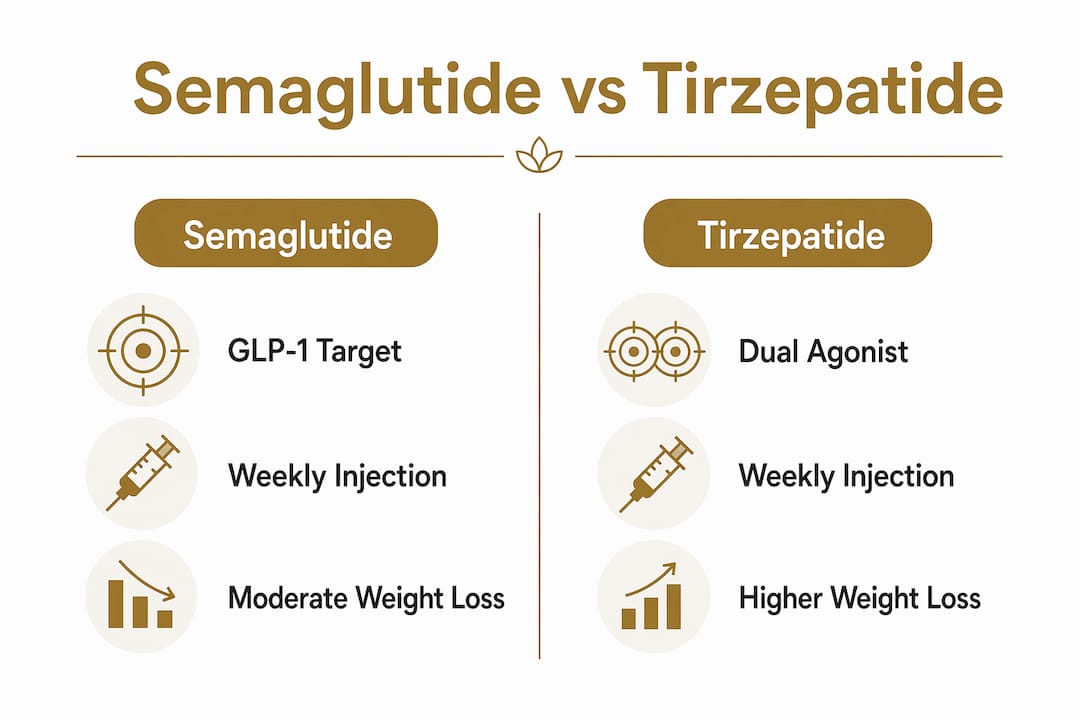
Tirzepatide adds a second layer. It activates both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors, producing synergistic appetite reduction and improved insulin sensitivity beyond what a single GLP-1 agonist achieves. Think of it as two hormonal levers pulled simultaneously instead of one. This dual mechanism is why tirzepatide’s clinical trial results exceed semaglutide’s in head-to-head comparisons.
- GLP-1 receptor agonism: suppresses appetite, slows gastric emptying, increases insulin secretion
- GIP receptor agonism (tirzepatide only): amplifies insulin sensitivity and energy expenditure
- Combined effect: greater caloric reduction, improved metabolic markers, sustained fat loss over months
Pro Tip: If you have type 2 diabetes or insulin resistance alongside obesity, the dual-agonist mechanism of tirzepatide may offer metabolic advantages beyond weight loss alone. Discuss this with your prescribing clinician before defaulting to semaglutide.
What does a typical peptide weight loss protocol look like in practice?
The protocol is structured, not open-ended. Every legitimate peptide weight loss regimen follows a dose escalation schedule designed to let your body adapt before reaching a therapeutic maintenance dose. Rushing this process is one of the most common mistakes patients make, and it reliably causes the gastrointestinal side effects that lead people to quit.
Here is how a standard semaglutide protocol unfolds:
- Week 1 through 4: Start at 0.25 mg subcutaneous injection weekly. This is a tolerability dose, not a therapeutic one. Do not expect significant weight loss here.
- Week 5 through 8: Escalate to 0.5 mg weekly. Appetite suppression begins to register for most patients.
- Week 9 through 12: Move to 1.0 mg weekly if tolerated. This is where consistent caloric reduction typically kicks in.
- Week 13 onward: Continue escalation toward maintenance doses of 1.7 or 2.4 mg weekly based on response and tolerability.
Tirzepatide follows a similar logic. Starting at 2.5 mg weekly, the dose increases in 2.5 mg increments every four weeks, with a maximum of 15 mg weekly. The escalation timeline for tirzepatide typically spans 20 weeks to reach full therapeutic dose.
Lifestyle integration is not optional. Both Wegovy and Zepbound are FDA-labeled as adjuncts to a reduced-calorie diet and increased physical activity. Patients who treat the injection as a standalone fix consistently underperform compared to those who pair it with a structured peptide diet plan. Clinical trials achieving 15 to 17 percent body weight loss did so with lifestyle modification built into the protocol from day one.

Duration matters too. Most peptide weight loss protocols run for a minimum of 68 weeks to achieve maximal outcomes, as demonstrated in the STEP and SURMOUNT-1 trials. Weight regain is common after stopping, which means your clinician should discuss long-term strategy before you start, not after you plateau.
Semaglutide vs. tirzepatide: which peptide is right for you?
Both are FDA-approved for chronic weight management in adults with obesity or overweight plus a weight-related condition. The differences lie in mechanism, efficacy data, and safety profile.
| Feature | Semaglutide (Wegovy) | Tirzepatide (Zepbound) |
|---|---|---|
| Receptor targets | GLP-1 only | GLP-1 + GIP (dual agonist) |
| Starting dose | 0.25 mg weekly | 2.5 mg weekly |
| Maintenance dose | 2.4 mg weekly | 5–15 mg weekly |
| Mean weight loss | ~15–17% at 68 weeks | ~17.8% at 72 weeks |
| Key contraindication | Personal/family history of MTC | Personal/family history of MTC or MEN 2 |
| FDA approval year | 2021 | 2023 |
The efficacy data from STEP and SURMOUNT-1 shows tirzepatide producing modestly greater average weight loss. That gap matters less than individual response, which varies based on genetics, baseline metabolic health, and adherence. Semaglutide has a longer real-world track record and more published long-term safety data as of 2026.
Both carry a boxed warning for thyroid C-cell tumor risk based on rodent studies. Tirzepatide’s FDA labeling includes contraindications for patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). This is not a theoretical risk to wave away. It is a hard stop that requires clinician screening before prescribing.
Common side effects for both include nausea, vomiting, diarrhea, and constipation, particularly during dose escalation. These are manageable with the correct titration schedule and dietary adjustments. Pancreatitis and gallbladder disease are rarer but documented risks that require monitoring.
Pro Tip: Do not select between semaglutide and tirzepatide based on marketing. Bring your metabolic labs, thyroid history, and GI history to your clinician and let the clinical picture drive the choice.
Safety considerations and medical oversight in peptide protocols
Peptide therapy for weight loss is not a self-directed experiment. Medical supervision is required because the risks are real, the contraindications are specific, and the dose escalation requires clinical judgment. Patients who source peptides outside of a licensed prescriber are bypassing the safety infrastructure that makes these protocols effective.
Before starting any protocol, a legitimate clinician will screen for:
- Personal or family history of MTC or MEN 2 (absolute contraindication for both agents)
- Active or history of pancreatitis
- Severe gastrointestinal disease
- Pregnancy or planned pregnancy
- Current medications that interact with GLP-1 agonists, particularly insulin or sulfonylureas
Monitoring during treatment is equally non-negotiable. Your provider should check in on gastrointestinal tolerability at each dose escalation, review any new symptoms that could indicate pancreatitis or gallbladder disease, and assess whether the current dose is producing the expected response. Dose holds or reductions are legitimate clinical tools, not failures.
“Contraindication screening for thyroid and endocrinologic risks is a crucial, non-negotiable component of any legitimate peptide protocol.” — Zepbound FDA Package Insert
The unregulated peptide market is a separate and serious problem. Many marketed “fat loss peptide stacks” lack clinical validation and carry regulatory and safety concerns that approved agents do not. Combining peptides without formal FDA approval or monitoring deviates from evidence-based practice and introduces unknown interaction risks. The highest-confidence protocols use approved agents at studied doses and durations. Everything else is speculation with your health.
Ongoing clinician follow-up is not bureaucratic overhead. It is the mechanism by which your protocol gets adjusted to your actual response rather than a population average. Patients who maintain regular provider contact achieve better outcomes and lower discontinuation rates.
Key takeaways
A peptide weight loss protocol works because it combines hormonal appetite regulation with structured dose escalation and lifestyle modification, not because any single injection produces fat loss on demand.
| Point | Details |
|---|---|
| Protocol definition | GLP-1 receptor agonists prescribed with diet and exercise, not standalone supplements. |
| Dose escalation is required | Semaglutide starts at 0.25 mg weekly; rushing escalation causes GI side effects and dropout. |
| Tirzepatide vs. semaglutide | Tirzepatide’s dual GLP-1/GIP mechanism produces slightly greater average weight loss in trials. |
| Safety screening is mandatory | Thyroid history, pancreatitis history, and drug interactions must be evaluated before starting. |
| Duration drives outcomes | Clinical trials achieving 15–17% weight loss ran 68–72 weeks with lifestyle integration. |
What I’ve learned from watching patients navigate these protocols
I have seen patients come in having already tried to self-titrate based on social media advice, and the pattern is almost always the same. They escalated too fast, got hit with nausea that lasted weeks, and concluded the medication “didn’t work for them.” The medication worked fine. The protocol was wrong.
The most underappreciated part of a peptide weight loss protocol is that the dose escalation schedule is not a suggestion. It is the difference between a patient who stays on therapy for 68 weeks and achieves meaningful fat loss, and one who quits at week six because they felt terrible. I have watched patients who followed the titration schedule precisely report almost no side effects at all. That is not luck. That is the protocol doing its job.
The other thing patients consistently underestimate is the lifestyle component. The GLP-1 receptor mechanism suppresses appetite, but it does not replace the need for a structured eating pattern. Patients who pair their protocol with a deliberate peptide diet plan, even a simple one, consistently outperform those who rely on reduced hunger alone to guide their intake.
My honest advice: treat this as a medical protocol, not a shortcut. The patients who get the best outcomes are the ones who show up to every check-in, report side effects honestly, and give the dose escalation the time it needs. The biology is on your side. The protocol is the vehicle. Do not skip steps.
— Amy
Start your peptide protocol with Revive-meds
If you are ready to move from researching to acting, Revive-meds offers clinician-supervised peptide therapy delivered to your door in 48 to 72 hours. Every protocol is reviewed by a licensed provider before anything ships, and all medications are US-compounded at FDA-registered pharmacies with 99%+ purity testing. There are no membership fees, no waiting rooms, and no generic plans.
Revive-meds builds your protocol around your labs, your history, and your goals. Whether you are exploring semaglutide for women or want to understand how GLP-1 therapy fits your specific metabolic picture, the process starts with a clinician conversation, not a checkout cart. Unlimited provider messaging and HSA/FSA eligibility are included. Learn more about how GLP-1 therapy works and take the first step toward a supervised protocol that is built for your body.
FAQ
What is a peptide weight loss protocol?
A peptide weight loss protocol is the prescribed use of GLP-1 receptor agonists like semaglutide or tirzepatide, combined with a reduced-calorie diet and physical activity, under clinician supervision. The protocol includes a structured dose escalation schedule and ongoing monitoring to maximize outcomes and minimize side effects.
How long does a peptide weight loss protocol take to work?
Most patients begin noticing appetite suppression within the first few weeks, but meaningful weight loss outcomes are measured at 68 to 72 weeks based on clinical trial data from the STEP and SURMOUNT-1 programs. Short-term results vary; the protocol is designed for sustained, long-term fat loss rather than rapid initial drops.
Are weight loss peptides safe without a prescription?
No. Peptides used outside of a licensed prescriber bypass contraindication screening, dose monitoring, and safety oversight that make these protocols effective and safe. Many unregulated peptide products lack clinical validation and carry unknown interaction risks.
What is the difference between semaglutide and tirzepatide for weight loss?
Semaglutide targets GLP-1 receptors only, while tirzepatide activates both GLP-1 and GIP receptors for a dual mechanism. Tirzepatide produces approximately 17.8% mean body weight loss at 72 weeks versus roughly 15 to 17% for semaglutide at 68 weeks, though individual response varies significantly.
Can you do a peptide weight loss protocol through telehealth?
Yes. Licensed telehealth clinics like Revive-meds provide clinician evaluation, prescription, and ongoing monitoring entirely online, with medications delivered directly to your home from FDA-registered compounding pharmacies.